-
Breast Cancer pathology
There are trillions of cells in the body. These cells have controlled cell cycle that controls their development, development, division, and demise. When they attain adulthood, the cells replicate to replace exhausted cells and to repair wounds. Cancer initiate when cells in a part of the body start to grow out of control. All types of cancer, irrespective of their origin, occur due to this uncontrollable growth of cells that leads to the formation of tumours and lesions. Cancer that develops from breast cells is known as Breast Cancer. Tumour formed by these cells can be seen on an x-ray or felt as a lump. When tumour cells grow into surrounding tissues or spread to distant areas of the body it become malignant. Breast cancer mainly occurs in women but man can also develop breast cancer, too. Breast cancer can develop from different parts of the breast. But most of the time the ducts that carry milk to nipple act as site for breast cancer. It may also start from the glands that make breast milk. Sarcomas and lymphomas are not really considered as breast cancer but they can also start from other tissues in the breast. Lump in the breast are not cancer but they are benign means they will not spread out, they are abnormal growths. But they can increase the risk for woman of getting breast cancer. When breast cancer cells enter blood or lymph system can spread the cancer and carry to the other part of the body. If the breast cancerous cells enter the lymph nodes it increases the chance of getting to spread to the other part of the body.
-
Breast Diseases:
There are several categories of breast diseases which may cause infections, cysts and lumps with or without pain. Some of the breast diseases are benign (harmless) and some are malignant (which can spread). Most common breast diseases are mastitis (a bacterial infection), cysts, benign lumps and cancer. Women mostly are affected by the breast diseases where they are encouraged to start breast self-examination early in the life and to have regular mammography, if found suspicious they are generally offered with a combination of ultrasound and needle biopsy to work out the cause. Men are affected by breast diseases too, although not as often.
-
Breast Cancer Grading and Staging
Staging and grading are ways in which healthcare professionals describe the size of your breast cancer, whether and how far it has spread, and how fast it may grow. Grading is Assess by evaluating acinar formation, nuclear size/pleomorphism and mitotic activity. An attempt should be made to grade the pre-operative core biopsy as there is acceptable concordance with excision grade.
Grading:
Grade 1 – the cancer cells look small and uniform like normal cells, and are usually slow-growing compared to other grades of breast cancer
Grade 2 – the cancer cells are slightly bigger than normal cells, varying in shape and are growing faster than normal cells
Grade 3 – the cancer cells look different to normal cells, and are usually faster-growing than normal cells
Staging: Staging is used to assess the size of a tumour, whether it has spread and how far it has spread. Understanding the stage of the cancer helps doctors to predict the likely outcome and design a treatment plan for individual patients.
Stage 1: Usually means that a cancer is relatively small and contained within the breast.
Stage 2 usually means the cancer has not started to spread into surrounding tissue but the tumour is larger than in Stage 1. Sometimes Stage 2 means that cancer cells have spread into lymph nodes close to the tumour.
Stage 3 usually means the cancer is larger. It may have started to spread into surrounding tissues and there are cancer cells in the lymph nodes in the area.
Stage 4 means the cancer has spread from where it started to another body organ. This is also called secondary or metastatic cancer.
Recurrent Breast Cancer: The cancer does return after treatment for early-stage disease, it is called recurrent cancer. When breast cancer recurs, it may come back in the following parts of the body, same place as the original cancer, chest wall, lymph node, bones, lungs, liver and brain.
-
Screening, Monitoring and Diagnosis
Breast Cancer can be detected through screening tests. Screening earlier can improve the chances of survival. Clinical breast exam, Biopsy and mammography are breast cancer screening tests. At higher risk of breast cancer breast MRI can also be used for some women. Powerful magnetic field and radio waves are used during Magnetic resonance imaging (MRI), which produces detailed images of structures within the breast. If breast cancer gets detected either by screening tests or from symptoms diagnostic tests are given to the woman who is suspected of having breast cancer.
Diagnostic tests includes Mammogram (X-ray of breast), Breast ultrasound (uses sound waves to produce pictures of structures), Removing a sample of breast cells for testing (biopsy), Breast magnetic resonance imaging (MRI).These diagnostic tests confirm the presence or absence of breast cancer and give more information about breast cancer like whether it has travelled outside the breast or not. Many tests are used to monitor how well therapies are working after the diagnosis of breast cancer.
-
Breast Pathology Treatment and Drugs
Breast cancer treatment team mainly includes Breast surgeon, surgical oncologist, radiation oncologist, medical oncologist, plastic surgeon. It also includes a variety of other health care professionals, including physician assistants, oncology nurses, social workers, pharmacists, counsellors, nutritionists, and others. The biology and behaviour of a breast cancer affects the treatment plan. Treatment options and recommendations are very personalized and depend on several factors, including: stage of tumour, tumour subtypes, genomic maker, patient age, and patient menopausal status, mutations in inherited breast cancer genes, such as BRCA1 or BRCA2. For both DCIS and early-stage invasive breast cancer, doctors generally perform surgery to remove the tumour. For larger cancers, or those that are growing more quickly, doctors may recommend systemic treatment with chemotherapy or hormonal therapy before surgery, called neoadjuvant therapy.
-
Breast Cancer Surgery
Breast surgery may be done for many causes, depending on the condition of the patient. Most women with breast cancer have some type of surgery as part of their treatment. Surgery may be done to remove the maximum cancer cells as possible (breast-conserving surgery or mastectomy) and to find out whether the cancer has spread to the lymph nodes under the arm (sentinel lymph node biopsy or axillary lymph node dissection) and/or restore the breast’s shape after the cancer is removed (breast reconstruction) and to relieve symptoms of advanced cancer.
-
Breast Cancer Pathology in Pregnancy
Breast cancer is found in about 1 in every 3,000 pregnant women. Breast cancer is the most common type of cancer found during pregnancy, while breastfeeding, or within the first year of delivery. You may hear this called gestational breast cancer or pregnancy-associated breast cancer (PABC). Sometimes due to hormonal changes in pregnancy, cancer may spread to lymph nodes. Pregnancy and breast feeding can also make breast tissue denser. Breast cancer may occur during the pregnancy and after the birth of child although the chances are less. Woman who is previously diagnosed with breast cancer and is now pregnant should take advice of consultant. Pregnancy is not a reason of breast cancer, but chances can be there in the women who are diagnosed from breast cancer. Treatment of breast cancer during the pregnancy depends upon size of tumour. Decisions should there between the consultant, surgeon and oncologist. And family support is also required at the same time.
-
Latest Advances and Innovative Therapeutic Approaches
Breast Pathology 2019 will be a chief interdisciplinary stage for the introduction of new advances and research results in the fields of Breast Cancer and Cancer Science. The meeting will unite driving scholastic researchers, analysts and researchers in the space of enthusiasm from around the globe. Topics of interest for submission include, but are not limited to:
-
Male Breast cancer
Breast cancer in men is a rare disease. Less than 1% of all breast cancers occur in men. Man, and women, girls and boys all have breast tissues. The various hormones in girls' and women's bodies stimulate the breast tissue to grow into full breasts. Boys' and men's bodies normally don't make much of the breast-stimulating hormones. As a result, their breast tissue usually stays flat and small. But sometimes men can develop real breast gland tissue because they take certain medicines or have abnormal hormone levels. In 2018, about 2,550 men are expected to be diagnosed with the disease. For men, the lifetime risk of being diagnosed with breast cancer is about 1 in 1,000.
-
Breast Cancer Prevention
Women may reduce their risk of breast cancer by maintaining a healthy weight, drinking less alcohol, being physically active and breastfeeding their children. Avoiding risk factors and increasing protective factors may help prevent cancer. The following are risk factors for breast cancer: Older age, A personal history of breast cancer or benign (no cancer) breast disease, A family history of breast cancer, Inherited gene changes, Dense breasts, Exposure of breast tissue to oestrogen, made in the body, Taking hormone, therapy for symptoms of menopause, Radiation therapy to the breast or chest, Obesity, Drinking alcohol.
-
Breast Cancer and Genetics
The two most common genetic risk factors for breast cancer are the BRCA1 & BRCA2 genes. Approximately 5% of all breast cancers are caused by a recognised specific genetic predisposition due to germ line mutations of one of two different genes: BRCA1 located on Chromosome 17q, BRCA2 located on Chromosome 13q. BRCA1 mutations also predispose to carcinoma of the ovary and possibly carcinoma of the Fallopian tube. The risk of developing breast cancer among carriers is around 55% by age 70. BRCA2: The product of BRCA2 is involved in controlling gene function and DNA repair. Gene function involves in transcriptional activation and completion of cell division by cytokinesis. Majority of BRCA2-associated tumours are invasive ductal, no special-type tumours.
-
Breast Pathology and Immunohistochemistry
Immunohistochemistry is a special staining process performed on fresh or frozen breast cancer tissue removed during biopsy. IHC is used to show whether or not the cancer cells have HER2 receptors and/or hormone receptors on their surface. This information plays a critical role in treatment planning. Immunohistochemistry (IHC) is used to characterize intracellular proteins or various cell surfaces in all tissues. Individual markers, or more often panels of various marker proteins, can be used to characterize various tumor subtypes, confirm tissue of origin, distinguish metastatic from primary tumor, and provide additional information which may be important for prognosis, predicting response to therapy, or evaluating residual tumor post-treatment. There is a growing list of available antibodies, which contribute to the broader utility of immunohistochemistry for solving diagnostic problems or for determining prognosis and response to therapy in breast pathology.
-
Case study and Case Reports
In medicine, a case report contains detailed report of the symptoms, signs, diagnosis, treatment, and follow-up of an individual patient. Case report usually describes an unusual or novel occurrence. Case reports are an unexpected association between diseases or symptoms. It may results in finding the shed new light on the possible pathogenesis of a disease or an adverse effect. It may contour Unique or rare features of a disease, unique therapeutic approaches.
-
Special Types of Breast Cancer
20% of breast carcinomas are of special type and the majority of these are lobular carcinomas. Tubular and mucinous carcinomas occur next most frequently and thereafter the remaining special types are seen infrequently. Special types of carcinoma should be distinguished from mixed carcinomas where the special type areas occupy between 50 and 90% of the tumour area with the remaining area being usually of no special type.
-
Women’s Health and Fitness
Breast health begins with a sense of what's normal for your breasts (breast awareness). To promote breast health, consider doing regular breast self-exams. For many women, breast health includes concerns about breast lumps, breast pain or nipple discharge. It's also important to understand common screening and diagnostic tests for breast health, such as clinical breast exams, mammograms and breast ultrasounds.
-
Nursing and Palliative care rehabilitation
The treatment and the cancer itself may affect the physical functioning and energy of the body. Life after breast cancer treatment gets changed like returning to some familiar things and new choices to make. After the last steps of treatment like radiation or diagnostic procedure is not the end of fighting against breast cancer. Physical energy and functioning can also be getting affected after the breast cancer treatment. Level of oestrogen may also get lowered after the treatment which leads to the decrease in bone density. Bone density can be increased as well recurrence of breast cancer can be prevented with the help of exercise. During oncology rehabilitation physical functioning as well as sense of well-being can be improved.
Oncology nurses are critical participants in the delivery of palliative care. It is the position of oncology nurse that primary nursing should begin at the time of diagnosis and continue throughout bereavement. Physical, psychological, social, cultural, and spiritual assessments are key components to the development of a comprehensive care plan for each patient. Oncology nurses must possess knowledge and skills in certain domains to deliver safe, quality palliative care including structure and processes of care, physical aspects of care, psychological care, and social aspects for care, cultural aspects of care, care of the imminently dying patient, ethical and legal aspects of care and, spiritual, religious, and existential aspects of care of a cancer patient. Oncology nurses have a responsibility to engage the public and provide fact-based information about care of people with advanced serious illness to encourage advance care planning and informed choices based on the needs and values of individuals.
-
Breast Cancer: Challenges, Breakthroughs
Breast cancer is the second most common cancer diagnosed after lung cancer and is the main cause of cancer demise in women. The heterogeneity of breast cancer such as ductal carcinoma in situ, triple negative breast cancer, HER2 negative among the women makes it difficult for the doctors to provide ideal medications for the cure. The major treatment methods are chemotherapy, radiation therapy, targeted drug therapy, oncoplastic surgery etc. Recent oncology research lead to the developments in neoadjuvant therapies, have also been benefited in treatment of breast cancer. Complete cure through Ayurveda was another major breakthrough in breast cancer treatment.
-
Breast Implants
There are three general types of breast implant devices, defined by their filler material saline solution silicone, silicone gel and composite filler. The saline implant has an elastomer silicones shell filled with sterile saline solution during surgery the silicone implant has an elastomer silicone shell pre-filled with viscous silicone gel and the alternative composition implant featured miscellaneous fillers such as soy oil, polypropylene string etc.
Market Analysis
Market Analysis of Breast Cancer
Breast cancer is a cancer that forms in the cells of the breasts. Breast cancer can occur in women and rarely in men. The symptoms of the breast cancer include a lump in the breast, bloody discharge from the nipple, changes in shape and size of the nipple or breast. There are 2 types of breast cancer: Non-invasive cancers stay within the milk ducts or lobules in the breast. They do not grow or invade in normal tissues within or beyond the breast. Non-invasive cancers are called as carcinoma in situ (in the same place) or pre-cancers. Invasive cancers do grow in normal, healthy tissues. Most breast cancers are invasive. Depending upon the type of cancer the treatment is determined, i.e., whether it is invasive or non-invasive cancer. Treatment varies depending upon the stage of cancer. It may consist of chemotherapy, surgery or radiation.
Early detection of breast cancer greatly increases the chances of successful treatment and saves the life. There are 2 major components of early detection of breast cancer: educate to promote early diagnosis and screening. There are 3 different types of screening tests available; they are the mammogram, clinical breast exam (CBE) and MRI (magnetic resonance imaging).
Is Breast Cancer a Modern Illness?
Ancient Egyptians were the first to diagnose, treat and prevent breast cancer more than 3,500 years ago. Breast cancer is now the most well-known and researched cancers in the medical world today. People diagnosed with breast cancer at an early stage have a very good chance of a cancer-free future. But this was not the case earlier. The first case of any type of cancer documented in Egypt was a breast cancer in 1600 BC. Edwin Smith Papyrus, an ancient text found in 1860 in an Egyptian tomb, described 8 cases of ulcers or tumors of the breast. The first doctor, who attempted to treat this type of cancer, wrote: “There is no treatment!” Physicians and medical researchers in ancient period posited the following theories regarding the cause of the breast cancer: humoralism, punishment, divine, lack of sexual activity, physical injuries, fear of breast cancer, without the benefit of 21st-century diagnostics. In ancient times, they used to call it “the wandering womb” where they believed that the uterus could move throughout the body leaving health problems of every kind in its wake. It was not diagnosed until the 19th century, unless and until the cases of breast cancer increased. But the disease is somewhat controlled with improvement in sanitation and hence the lifespan of an individual is increased.
The first successful treatment for breast cancer was done by French surgeon Jean Louis Petit and later Scottish surgeon Benjamin Bell where the lymph nodes, breast tissue, and chest muscle are removed surgically. Surgeon William Stewart Halsted began performing and perfecting mastectomies around 1882. Halsted’s mastectomies were invasive where breasts, lymph nodes, and underlying muscles are being removed and the procedure was deemed necessary to prevent cancer from recurring but often left patients with severe pain and disability.
By the 1970’s, researchers began to develop lumpectomy- more limited surgery to remove only the cancerous tumor and any surrounding tissue affected by the tumor.
By 1985, researchers found that radiation followed by lumpectomy gave a chance of survival equal to the considerably move invasive mastectomy.
Around the 20th century, doctors used radiation therapy to shrink the cancerous cells. Chemotherapy became an option. It helped to shrink cancerous cells before surgery and prevent recurrence after surgery and treat cancer that is metastasized or has spread to other parts of the body. Scientists began to experiment with combined treatments to improve outcomes. Throughout the 1970’s, this procedure has been continued and this led to a better understanding of how cancer can develop and spread throughout the body. This understanding led to the development of more effective targeted treatments. This approach to treat cancer and research is still continuing today.
In 1923, the first large-scale review of women with breast cancer was done by English scientist Janet Lane-Claypon, which identified several risk factors that are still considered today.
In 1980’s and 1990’s, thousands of women undergoing breast cancer treatment and high dose bone marrow transplants hoping to have a good result, which turned it to a disaster after the loss of 15-20% of women’s life due to the treatment.
In 1995 report from the Nurses’ Health Study and 2002 results of research from the Women’s Health Initiative concluded that hormone replacement therapies which had become popular among menopausal women could significantly increase the risk of breast cancer.
In the late 1990’s, scientists found that certain variants of the genes BRCA1 and BRCA2 are associated with 80% of breast cancer risk. Some women who discover this gene mutation within their genetic makeup will take proactive steps to reduce their risk of cancer, including preemptive mastectomies and even hysterectomies.
As scientists deepen their understanding of the role of genetics in breast cancer risk, research on developing new techniques has been increased. Meanwhile, some research is being done on repair or even replaces harmful genes before breast cancer occurs.
As research continues to improve, there are several chances of every person to survive and can prevent breast cancer or any type of cancer. Taking healthy food, avoiding alcohol and smoking may be an important precaution from developing cancer. Regular self-exams and annual mammograms after 40 years old are recommended.
What’s New in Breast Cancer Research?
Treatments are being evaluated in trails. This includes individual drugs, the combination of drugs, surgical and radiation techniques. Investigations include new types of cancer vaccines, targeted therapy, oncolytic virotherapy, and immunotherapy.
The latest research is reported annually at scientific meetings such as the American Society of Clinical Oncology, San Antonio Breast Cancer Symposium and St. Galen Oncology Conference, Switzerland. These studies are reviewed by professional societies and other organizations and formulated into guidelines for specific treatment groups and risk category.
Fenretinide, a retinoid (drugs related to vitamin A), is also being studied as a way to reduce the risk of breast cancer.
Cryoablation
As of 2014, cryoablation is being studied to see whether it could be the subtitle for lumpectomy in small cancers. There is tentative evidence in those with tumors less than 2 centimeters. It can also be used for those, surgery is not possible. Another review stated that cryoablation looks promising for early breast cancer of small size.
Breast cancer cell lines
A considerable part of the current knowledge on breast carcinomas is based on in vivo and in vitro studies, performed with cell lines derived from breast cancers. These provide an unlimited source of homogenous, self-replicating material, free of contaminating stromal cells and often easily cultured in simple standard media. The first breast cancer line described was BT-20, established in 1958. Since then, despite sustained work in this area, the number of permanent lines obtained has been strikingly low. Indeed, attempts to culture breast cancer cell lines from primary tumors have been largely unsuccessful. This poor efficiency was often due to technical difficulties associated with the extraction of viable tumor cells from their surrounding stroma. Most of the available breast cancer lines issued from metastatic tumors, mainly from a pleural effusion. Effusions provided generally large numbers of dissociated, viable tumor cells with little or no contamination by fibroblasts and other tumor stroma cells. Many of the currently used BCC lines were established in the late 1970’s. a very few of them, namely MCF-7, T-47D, and MDA-MB-231, account for more than two-thirds of all abstracts reporting studies on mentioned breast cancer cell lines, as concluded from a Medline-based survey.
Molecular markers
Transcription Factors
NFTA transcription factors are implicated in breast cancer, more specifically in the process of cell motility at the basis of metastasis formation. Indeed, NFAT1 (NFATC2) and NFAT5 are pro invasive and promigratory in breast carcinoma and NFAT3 (NFATC4) is an inhibitor of cell motility. NFAT1 regulates the expression of the TWEAKR and its ligand TWEAK with the Lipocalin 2 to increase breast cancer cell invasion and NFAT3 inhibits Lipocalin 2 expression to blunt the cell invasion.
Metabolic markers
Clinically, the most useful metabolic markers in breast cancer are the estrogen and progesterone receptors that are used to predict response to hormone therapy. New or potentially new markers for breast cancer include BRCA1 and BRCA2 to identify patients at high risk of developing breast cancer, HER2 and SCD1 for predicting response to therapeutic regimens and urokinase plasminogen activator, PA1-1 and SCD1 for assessing prognosis.
Survey Report
Breast cancer is the second leading cancer in women worldwide, with nearly 1.7 million new cases diagnosed in 2012. Breast cancer is most common after menopause. American Cancer Society, for the year 2016 estimates that about 252,710 new cases of invasive breast cancer will be diagnosed in women, about 63,410 new cases of carcinoma in situ (CIS) will be diagnosed and about 40,601 women will die from breast cancer.
Trends in breast cancer incidence
Incidence rates vary from 19.3 per 100 000 women in Eastern Africa to 89.9 per 100 000 women in Western Europe and are high in developed regions of the world (more than 80 per 100 000) except Japan and low in most of the developing regions (less than 40 per 100 000). Although developed countries have high incidence rates, in the transition countries like Latin America, it is going to be increased in the future. The rates vary worldwide, with Europe being the highest. The rates are increasing in Latin America and Asian countries mainly due to the population aging and screening practices.
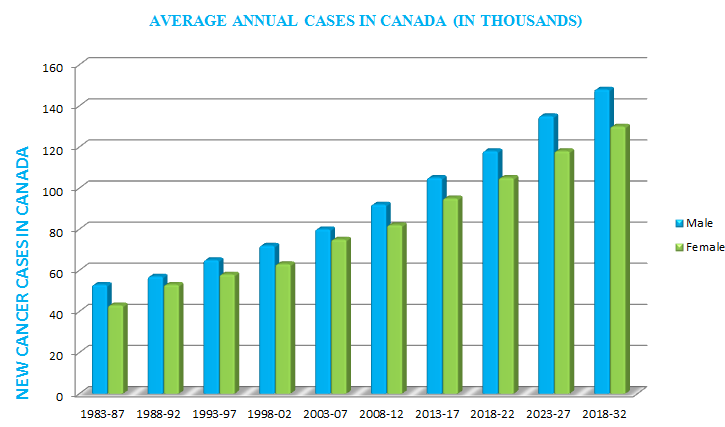
The total number of cases registered for five year period 1998-2002 were 13 120 964 (6 848 973 men and 6 271 991 women), the average of annual cases registered to be about 1 250 000 for women and 1 369 795 for men. During this period, 1 775 353 cases of breast cancer were registered worldwide. The highest rates occurred in Europe (Belgium, France, Switzerland, Italy) and in Australia with average rates of 60-100/100 000 cases. The lowest ASR (W) was between 18-30/100 000 in India, Thailand, China and Africa (Harare and Kyadondo).
Canada Breast Cancer Statistics
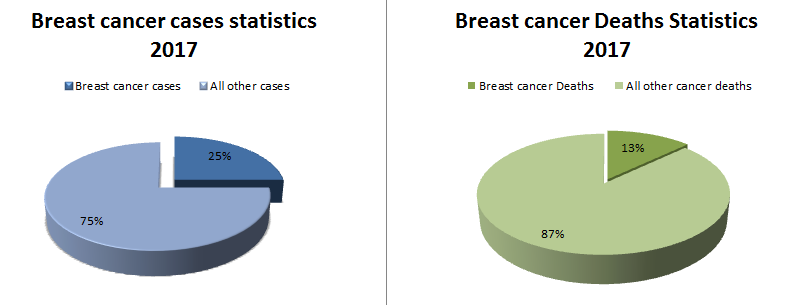
26,300 women were diagnosed with breast cancer. This represents 25% of all new cancer cases in women in 2017. 5,000 women died from breast cancer. This represents 13% of all cancer deaths in women in 2017.
On average, 72 Canadian women were diagnosed with breast cancer every day. On average, 14 Canadian women died from breast cancer every day. 230 men were diagnosed with breast cancer and 60 died from breast cancer.
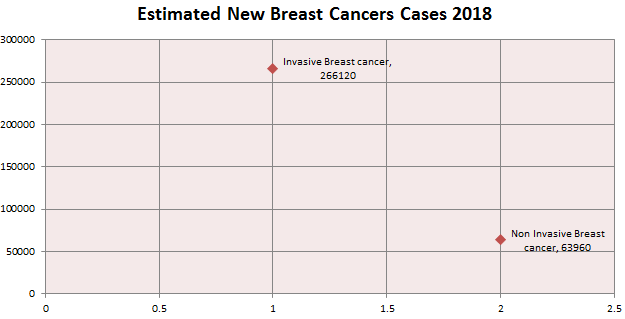
About 12% of Canadian women (1 in 8) will develop breast cancer over the course of her lifetime. In 2017, an estimated 266,110 new cases of invasive and 63,960 new cases of non-invasive (in situ) breast cancer are expected to be diagnosed.
After increasing incidence rates of breast cancer for the previous two decades, it began decreasing in the year 2000 and dropped by 7% from 2002 to 2003 alone. This decrease was partially due to the reduced use of hormone replacement therapy (HRT) by women after results of a large study called Women’s Health Initiative which was published in the year 2002. These results suggested a relation between HRT and increased breast cancer risk.
Though death rates have been decreased since 1989, about 40,610 women are expected to die in the year 2017 in the U.S. from breast cancer. Women under the age of 50 have experienced larger decreases. These decreases are thought to be the result of treatment advances, earlier detection through screening and increased awareness.
Besides skin cancer, breast cancer is the most commonly diagnosed cancer among American women. In 2017, it is estimated that about 30% of new cases diagnosed in women will be breast cancers.
Breast cancer is more common in African-American women than in white women under the age 45. Overall, African-American women are more likely to die of breast cancer. For Asian, Hispanic and Native-American women, the risk of developing and dying from breast cancer is lower. As many as 40 % cases more cases are predicted by 2030.

The risk of breast cancer in women doubles, if she has a first-degree relative (mother, sister or daughter) who has been diagnosed with breast cancer. Less than 15% of women who get breast cancer have a family member diagnosed with it.
About 5-10% of breast cancer is linked to gene mutations (abnormal changes) inherited from one’s mother or father. Mutations of BRCA1 and BRCA2 genes are the most common ones. On an average, women with the BRCA1 mutation have a 55-65% lifetime risk of developing breast cancer. The risk is 45% for the women with the BRCA2 mutation. Breast cancer that is positive for the BRCA1 and BRCA2 mutations tends to develop more often in younger women. An increased ovarian cancer risk is also associated with these genetic mutations. In men, BRCA2 mutations are associated with a lifetime breast cancer risk of about 6.8%, BRCA1 mutations are a less frequent cause of breast cancer in men.
The objective behind the Conference
The main objective of holding Breast Pathology and Cancer Diagnosis 2019 conference is to share the latest research and developments of individuals in the sphere of cancer, which helps to develop new techniques for the treatment and can also discuss and plan to reduce the use of chemotherapy treatment by introducing special drugs that will continue to develop and directly attack special targeted breast cancer cells.
Pharmaceutical Companies Leading the Breast Cancer Fight
-
Bristol-Myers Squibb Co. (NYSE: BMY)
-
Merck & Co. Inc. (NYSE: MRK)
-
Medivation Inc. (NASDAQ: MDVN)
-
Pfizer Inc. (NYSE: PFE)
Breast Cancer Associations & Societies around the Globe
1. American Cancer Society
2. American Medical Women's Association
3. American Society for Radiation Oncology
4. American Society of Paediatric Hematology/Oncology
5. Association of Cancer Physicians
6. Association of Chartered Physiotherapists in Women’s Health
7. Association of Women's Health, Obstetric and Neonatal Nurses
8. Breast Screen Australia Program
9. Cancer Relief Society Nepal
10. Cancer Society of Finland
11. Cancer Society of New Zealand
12. Caribbean Women's Health Association
13. European Association for Cancer Research (EACR)
14. Indonesian Society of Gynecologic Oncology
15. International Association for Women's Mental Health
16. International Gynecologic Cancer Society
17. Iranian Society of Radiation Oncology
18. Japanese Breast Cancer Society
19. New Zealand Breast Cancer Foundation (NZBCF)
20. Society for Women's Health Research
21. Spanish Association for Cancer Research (CMA)
22. Thai Gynecologic Cancer Society